|
|
|
||
| Home | About | Donate/Volunteer | Contact | Jobs| |
|
|
New Treatments for Schizophrenia Stanford University Schizophrenia and Bipolar Education Day, July 30 2005 | ||||||||||
|
Lecture Outline:
Editor's Note: the following is a summary of a lecture given by Dr. Ira Glick, Professor of Psychiatry at the Stanford University School of Medicine. Direct quotes will be indicated with quotation marks; any other text is paraphrase based on Dr. Glick's words.
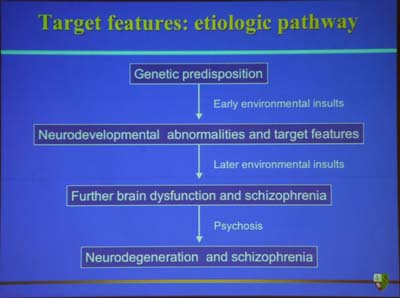
Dr. Glick opened his talk on new treatments for schizophrenia with the above quote, attributed to his colleague Dr. William Carpenter. He interpreted this to mean that there is always hope for the person with schizophrenia . This is especially true today, with newer and better treatments becoming available all the time. Dr. Glick presented one possible etiologic (causal) path to schizophrenia that has many levels for potential intervention and reversal - see the diagram below:
The above is not necessarily an inevitable path from beginning genetic vulnerablity to eventual schizophrenia, Dr. Glick emphasized; the etiologic flowchart is an "interactive model", which has room for interventions at every level. However, "if one does these things [environmental insults such as substance abuse], and has a vulnerability, you get further brain disfunction and neurodegeneration - in plain language, losing brain cells. You have less cells to work with as you go through life, putting you at a severe disadvantage." Dr. Glick also presented a hopeful picture of the natural course of schizophrenia; namely, that it has a tendency to stabilize with age. After the first "psychotic break", which generally happens in the early 20s, the severity of symptoms seem to stabilize somewhat after about age 30 or so. However, the importance of early intervention and treatment is crucial, because there is "ongoing damage to the brain." As his early-intervention method of choice, Dr. Glick promotes the use of second-generation antipsychotics, always in conjunction with psychosocial intervention and work with the family. "The earlier you treat with second-generation antipsychotics, the better your chances at reducing the possibility of a full blown psychosis." And hopefully, if the etiology flowchart above is anything to go by, the better your chances at reducing neurodegeneration and chronic schizophrenia. First-Generation (FGA) vs. Second-Generation (SGA) Antipsychotics According to Dr. Glick, "we are significantly better off than we were twenty years ago, especially in terms of reduced side effects." This state of affairs, he believes, is largely due to the introduction of second-generation (or atypical) antipsychotics, most of which have been approved only within the last five years. Data cited by Dr. Glick indicated that the atypical antipsychotics were better for reduced side effects, suicide prevention (esp. clozapine), and for treatment-resistant cases (esp. clozapine, and polypharmacy combinations). He showed this in a major meta-analysis of the first-generation vs. the second generation antipsychotics (Davis, Chen, and Glick, 2003), contrasting with earlier findings by Geddes et al (2000), who concluded that the earlier and later classes of drugs were about equal in efficacy. Unfortunately, many public insurance plans use data such as Geddes' as a reason to exclude the more expensive atypical antipsychotics from their approved drug lists. Glick reiterated that he did not believe that the first-generation drugs were equal to the second-generation drugs in terms of efficacy and side effect control. Dr. Glick also emphasized the importance of treating all aspects of a schizophrenia-specturm disorder. "[Treatment] is manifested not just in what people are focusing on - the voices, the delusions, the moods. The key area is the negative symptoms. And the key prognostic of what the future will bring is how well we treat these negative symptoms - memory, attention, executive function, how to get yourself through the day." In terms of a prognostic outlook today, Dr. Glick estimated that about 10% of people with schizophrenia look "totally normal" - that is, you couldn't distinguish them from a healthy person out of the general population. Getting to this phase of long-term recovery depends on several things:
One of the major barriers to any of these three aspects of treatment is patient compliance. Studies show that non-compliance with psychiatric medication is a major reason for relapse, and is strongly influenced by patients' attitudes towards treatment (Editor's Note: see schizophrenia.com Newsblog entry from July 7, 2005 for more research on this topic ). An important factor that can positively or negatively influence a patient's attitude towards medication (the studies show), is that patient's relationship with his/her doctor. Dr. Glick would seem to agree. He cited data from one study indicating the following things that patients want from a doctor-patient relationship:
Helping an ill relative (or helping yourself) find a doctor with whom you can develop such a relationship may vastly improve attitudes towards treatment, reducing the chances of relapses and improving the overall prognosis of the disease course. (Editor's note: click here for resources on how to find a good psychiatrist) In summary, Dr. Glick drew the following conclusions concerning schizophrenia treatment:
|
Advertisement
|